
Patient AR and insurance AR are different problems, and they demand different solutions. This article focuses exclusively on patient accounts receivable; the balances patients owe after insurance has paid its portion. Insurance payers have regulatory obligations and structured reimbursement timelines. Patients do not. Everything below is about collecting patient balances at the point of care, before time works against you.
Most healthcare practices spend the majority of their billing resources managing insurance claims. And while insurance AR matters, it always eventually pays. Patient AR is a different story.
Once a patient leaves your office without settling their balance, the odds of collecting drop fast. According to CMS data, claims that age past 120 days have less than a 15% chance of collection. After a year, collection probability approaches zero. In fact, providers today collect just 24% of patient billings after insurance.
That urgency is compounded by how far industry-wide patient collection rates have fallen, from 54.8% in 2021 to just 34.4% in 2024. Providers are now collecting barely one-third of what patients owe. A 2025 MGMA poll of 247 medical group leaders found that 40% report patient balance collections about the same as last year, and 26% report better. So, the window to act is narrower than most practices realize, and it opens and closes within a single visit.
Patient AR vs. Insurance AR: Understanding the Difference
Before going further, it's worth being explicit about the distinction because most practices treat them as variations of the same problem, when they are not.
Insurance AR is a process problem. If you manage the claims lifecycle correctly, you will collect most of it. While patient AR is a timing problem, the window is open while the patient is in front of you, and it starts closing the moment they leave.
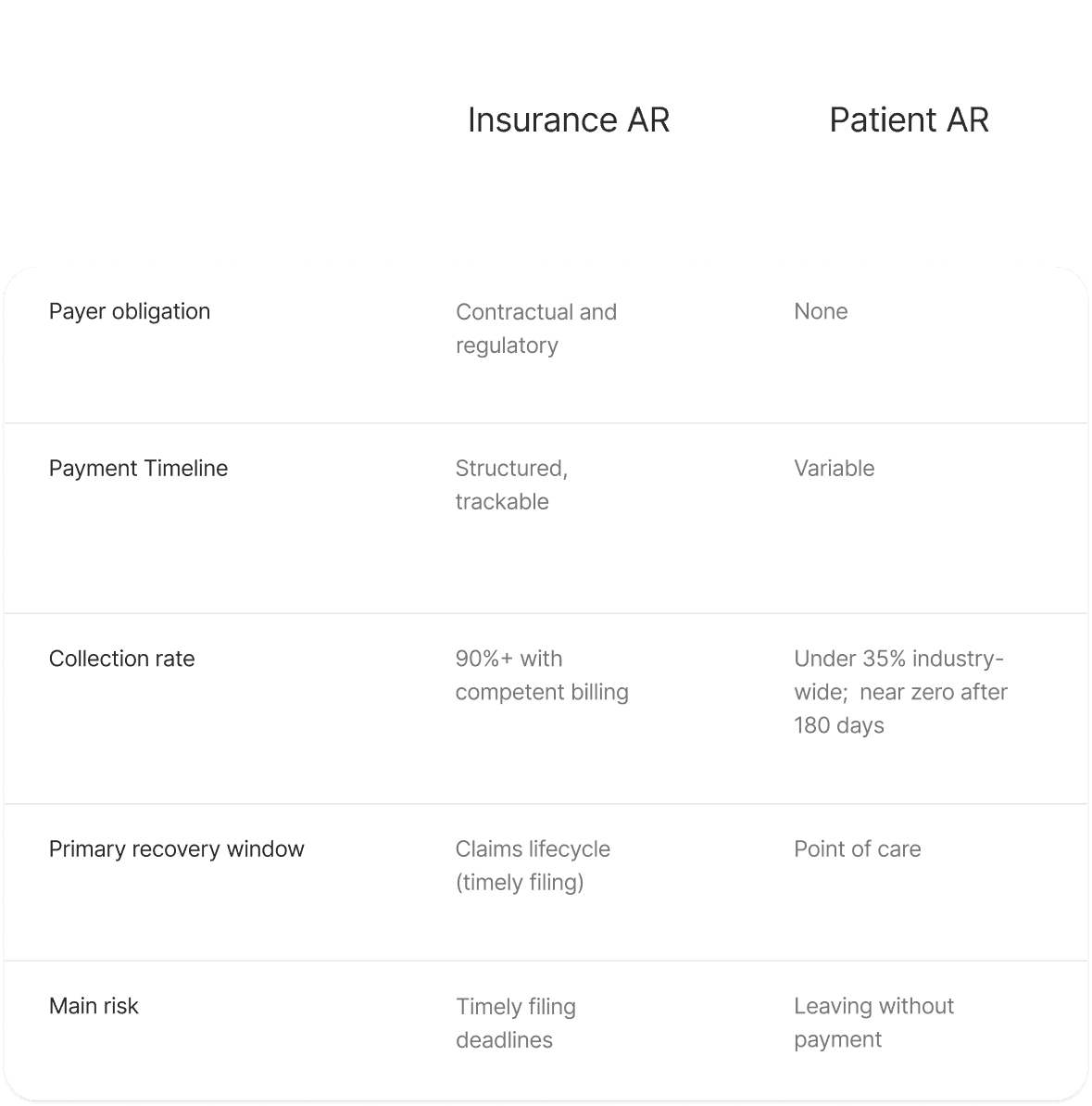
The strategies for each are almost entirely different. Denial management, claim scrubbing, and payer follow-up are insurance AR tools. Good faith estimates, checkout conversations, cards-on-file, and post-remittance automation are patient AR tools. Treating them the same way means handling neither effectively.
Why Collecting Patient Payment AR is Getting Harder
The shift toward high-deductible health plans has fundamentally changed who your most challenging payer is. According to the U.S. Bureau of Labor Statistics, 51% of private industry workers were enrolled in high-deductible health plans in 2023. The median annual deductible for those plans was $2,750. As deductibles climb, so does the portion of every bill that lands in the patient's lap. The patient is now, in many cases, your largest single-balance payer and the one with the least structured obligation to pay.
Most practices still operate with billing infrastructure built for insurance reimbursement. They are using the right tools for the wrong payer.
4 Reasons Patient AR Keeps Growing
Patient AR almost always traces back to the same four failure points. Here is what drives each one, and the specific fix that addresses it:
1. Unclear Patient Financial Responsibility
If a patient does not know what they owe before their appointment, they cannot prepare to pay it. Without an upfront cost estimate and a clear explanation of their financial responsibility, many are surprised when a bill arrives weeks later. That often leads to payment delays, disputes, and higher patient accounts receivable (AR).
2. No payment structure at checkout
The most common patient AR mistake is letting patients leave without a defined payment agreement. This does not mean demanding full payment at the door. It means ensuring every patient leaves with one of three things: a payment in full, a card-on-file with a scheduled charge, or a payment plan with agreed terms.
Point-of-service collections are more successful than post-visit billing when patients are provided upfront cost estimates and clear payment options. “We'll send you a bill” is not a collection strategy.
3. Relying on Patient Billing Statements
The traditional patient billing cycle is expensive and largely ineffective. Even after multiple billing reminders, healthcare organizations frequently recover only a part of outstanding balances.
By the time a balance hits 90 days, collection probability has already dropped by half.
4. Delayed Patient Billing After Insurance
Insurance payment and patient balance are often treated as separate events. The insurance pays. Someone manually reviews the remittance, and then the patient statement goes out. Each handoff introduces delay, and delay kills collection rates.
4 Proven Strategies to Reduce Patient AR Days
The strategies that move the needle on patient AR are about structuring the patient encounter so that collection happens at or before the point of care.
1. Deliver Good Faith Estimate
Under the No Surprises Act, practices are required to provide Good Faith Estimates for uninsured and self-paying patients, with the requirement considered to be expanding to insured patients as well. Either way, the operational value extends well beyond compliance.
A good faith estimate delivered before treatment does three things:
Gives the patient time to prepare financially
Removes the element of surprise that causes disputes and delays
Creates a documented expectation that supports the checkout conversation
Practices that build this into their standard intake workflow report fewer billing disputes and faster patient payment
2. Present payment options at checkout
Every patient who completes a visit should leave having chosen one of the following:
Pay the estimated balance in full
Place a card-on-file to be charged when the final balance is confirmed
Enroll in a payment plan with defined terms
The key word is chosen. Patients who actively select a payment option are dramatically more likely to follow through than those who receive a passive statement later.
3. Automate post-remittance action
When insurance pays, the remaining patient´s balance should not sit in a queue. The action should be automatic.
If the patient placed a card on file, charge it. If they are enrolled in a payment plan, initiate it. If they opt for an invoice, send it immediately. This single operational change connects the insurance payment event directly to patient balance action.
4. Track patient AR separately from insurance AR
Track patient AR as its own metric, so you can see clearly where the problem is and measure improvement over time.
Key indicators to monitor:
Patient AR aging buckets — 0–30 days is healthy; 61–90+ days signals a breakdown in the checkout or post-remittance workflow; 180+ days approaches unrecoverable.
Point-of-care collection rate — the percentage of patient responsibility collected at or before checkout; this is your leading indicator
Patient collection rate — the industry benchmark has fallen to 34.4%; your own rate tells you exactly where you stand relative to peers
Bad debt rate — above 5% means you need to collect more upfront
How Patient AR-Focused Revenue Cycle is Addressed
The difference between a practice with 62 days in AR and one with 35 days often comes down to one thing: how early a patient encounters the financial conversation.
A best-practice patient AR workflow:
Before the visit: Eligibility is verified in real time. The patient receives a good faith estimate with their out-of-pocket responsibility clearly stated.
At check-in: Staff confirm the patient has reviewed their estimate and addressed any questions about financial responsibility.
Checkout: The patient selects a payment option, for example full payment, card-on-file, or a payment plan. A commitment is secured before they leave.
After insurance pays: The system automatically acts on the patient's pre-selected option. No manual review delay. No statement sitting in a print queue.
Ongoing: Patient AR is tracked separately, with aging buckets reviewed regularly. Any balance approaching 60 days triggers a defined escalation workflow. Myriad Systems unifies eligibility verification, estimate generation, payment options, AI-assisted coding, and post-remittance workflows on a single platform. Patient balances can be addressed before checkout, while insurance-related follow-up actions happen automatically.
Ready to see what your patient AR recovery rate could look like? Schedule a free consultation with our team to walk through your current workflow and identify where patient balances are slipping through.





